I know I haven’t mentioned lymphodema (‘lymphedema’ if you’re American) on here in a while, but it’s a topic of conversation that happens quite often in clinic.
There are different types of lymphoedema and for many people conservative management (e.g. compression, lymphatic drainage – either manually or using Endermologie, compressive pumps etc.) is the mainstay of treatment. But, some people may be candidates for surgery.
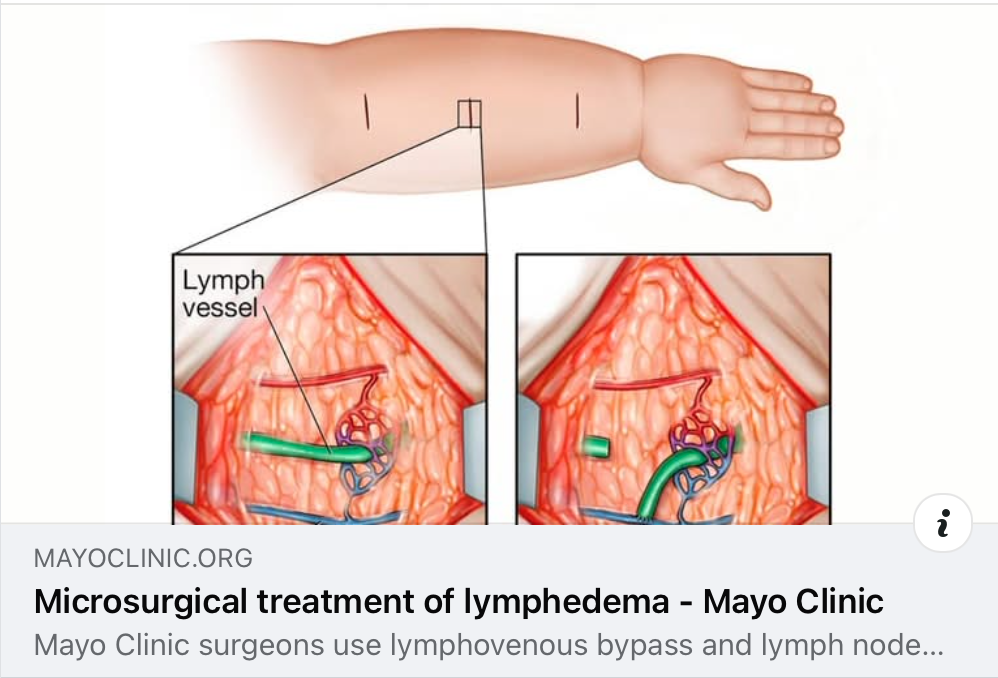
This is a long-winded way to say, if you, or anyone you know has lymphoedema, this article explains how this lymphovenous bypass (LVB) or vascularised lymph node transfer (VLNT) surgery can restore lymphatic flow and drainage in some people with lymphedema.
You can read the article by clicking on the link here:
If you don’t have time, here’s a quick summary:
- Context: Lymphedema is a chronic condition typically managed by conservative therapies like compression, manual lymphatic drainage, and skin care. These help reduce swelling and infection risk but require ongoing daily effort.
- Surgical options: When conservative approaches aren’t sufficient, surgical interventions – either liposuction (for debulking) or microsurgical reconstruction – can provide more durable relief.
- Microsurgery techniques:
- Lymphovenous bypass (LVB): Surgeons connect tiny lymphatic vessels to nearby veins using supermicrosurgical tools and magnification up to 40×. It’s minimally invasive, usually outpatient, with expected limb volume reduction of ~20–30% within one year post‑surgery.
- Vascularized lymph node transfer (VLNT): Healthy lymph nodes (and their blood vessels) are transplanted from donor sites—such as abdomen, groin, back, or chin—to the affected limb. This is more invasive and often used when bypass isn’t feasible. Studies show improved outcomes months after surgery, including reduced cellulitis by a factor of 10, pain relief in 75% of patients, and 42% discontinuation of compression garments.
- Considerations: Ideal candidates are those who haven’t responded adequately to conservative care. Obesity, untreated venous insufficiency or deep‑vein thrombosis, and previous treatment noncompliance may limit eligibility.
- Research and outcomes tracking: Mayo Clinic continues to study timing, number of bypasses, surgical modes, and their impact on outcomes. The goal is to optimise patient selection and efficacy of these advanced treatments.
Bottom line
Microsurgical treatments like LVB and VLNT offer a regenerative, long‑lasting alternative when traditional lymphedema therapies fall short. LVB is minimally invasive and often effective in early stages, while VLNT may deliver substantial benefit even when bypass is not viable. Ongoing research at Mayo Clinic aims to refine which patients benefit most and improve long‑term outcomes.